Providing an Exceptional Patient Experience
Welcome, where exceptional patient experiences are our priority. With compassionate care, state-of-the-art facilities, and a patient-centered approach, we're dedicated to your well-being. Trust us with your health and experience the difference.

Our Special Service
Beyond simply providing medical care, our commitment lies in delivering unparalleled service tailored to your unique needs. And we mean it!
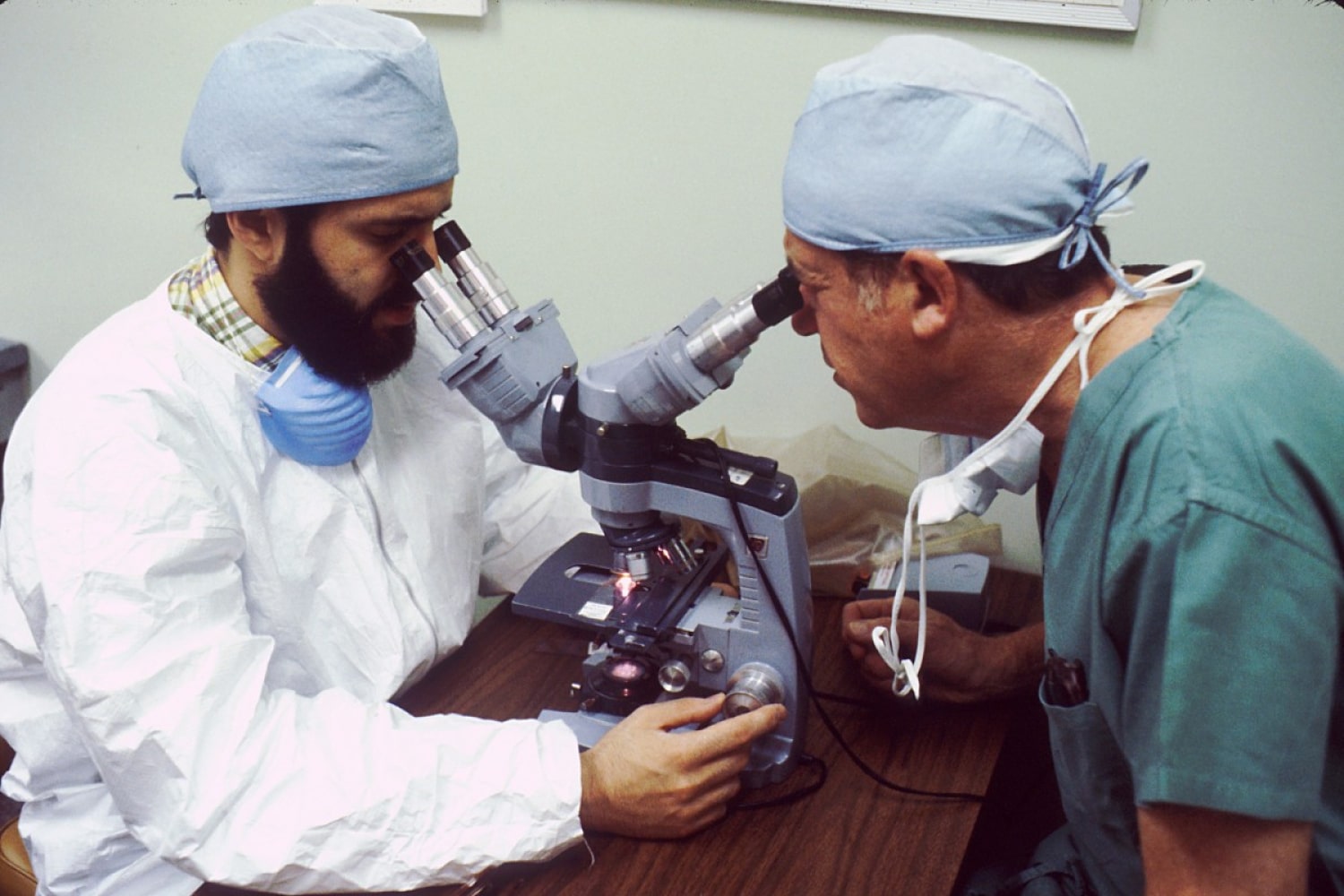
Laboratory Test
Accurate Diagnostics, Swift Results: Experience top-notch Laboratory Testing at our facility.
Health Check
Our thorough assessments and expert evaluations help you stay proactive about your health.
General Dentistry
Experience comprehensive oral care with Dentistry. Trust us to keep your smile healthy and bright.
About Us
Welcome to our healthcare website, your one-stop destination for reliable and comprehensive health care information. We are committed to promoting wellness and providing valuable resources to empower you on your health journey.
Explore our extensive collection of expertly written articles and guides covering a wide range of health topics. From understanding common medical conditions to tips for maintaining a healthy lifestyle, our content is designed to educate, inspire, and support you in making informed choices for your health.
Discover practical health tips and lifestyle advice to optimize your physical and mental well-being. We believe that small changes can lead to significant improvements in your quality of life, and we're here to guide you on your path to a healthier and happier you.


Why Choose Us
With a steadfast commitment to your well-being, our team of highly trained healthcare professionals ensures that you receive nothing short of exceptional patient experiences.
Intensive Care
Our Intensive Care Unit is equipped with advanced technology and professional team.
Free Ambulance Car
A compassionate initiative to prioritize your health and well-being without any financial burden.
Medical and Surgical
Our Medical and Surgical services offer advanced healthcare solutions to address medical needs.
Our Special Doctors
We take pride in our exceptional team of doctors, each a specialist in their respective fields.
Dr. James Anderson
Cardiologist

Dr. Emily Smith
Neurosurgeon

Dr. William Johnson
Dermatologist